

What Gets Adopted, And Who Decides?

You haven’t heard from me for a couple of weeks.
I’ve been in the United States attending conferences, meeting practitioners, and speaking with researchers about Q Magnets. Including Professor Dr Pradip Ghosh and final-year physiotherapy students at Maryville University in Saint Louis, MO.

Those conversations were encouraging, but they also brought me back to a bigger question I’ve been thinking about for years:
Why do ordinary ideas get adopted quickly, while others struggle to be taken seriously, even when they may have genuine value?
That question matters for Q Magnets.
It matters for healthcare.
And, as history shows, it matters far beyond medicine.
A system doesn’t always choose what works best
One of the things I’ve noticed from my many trips to the United States is how influence operates within their political system.
I don’t say that as a partisan comment. It is about structure.
The United States has a highly developed lobbying system where large industries, wealthy donors, and powerful interest groups often have direct access to the people writing legislation. In 2024, federal lobbying spending in the US reached a record US$4.4 billion, according to OpenSecrets.
That doesn’t mean every decision is corrupt.
But it does mean access is not evenly distributed.
If an industry has money, lobbyists, political relationships, and a strong commercial interest in maintaining the status quo, it has a much greater chance of shaping policy than a smaller idea, a less profitable solution, or an intervention that doesn’t fit neatly into the existing system.
In healthcare, this becomes especially important.
Some interventions don’t struggle because they are useless.
They struggle because they do not have the lobbying power behind them.
Or because they might disrupt vested interests that already have influence.
Or because they are difficult to patent, package, scale, and sell in the way the system prefers.
Trams are a useful example
A simple way to see this is through transport.
Most major American cities once had tram or trolley systems. Many were removed. Roads expanded. Cars became dominant.
This video gives a useful overview of the American trolley story:
US — The Real Reason America Killed Its Trolley Systems
My home city of Melbourne took a different path.
Melbourne kept its trams.
This video explains that story:
Australia — Why did Melbourne keep its trams?
That outcome wasn’t inevitable. It happened because individuals resisted the pressure to follow what other cities were doing.
One of those people was Major General Sir Robert Risson, chairman of the Melbourne and Metropolitan Tramways Board from 1949 to 1970. He is widely recognised as a major reason Melbourne retained its tram network at a time when trams were falling out of favour.
The point is not that trams are perfect.
The point is that what survives is not always what is objectively best.
Often, it is what powerful interests lobby to remove, or what someone courageous decides to protect.
Not everyone gives in to the system
Clair Patterson is an important example.
Patterson was the American geochemistry who helped determine the age of the Earth. But in doing so, he also uncovered widespread environmental lead contamination.
His work eventually challenged the use of lead in petrol, paint, food containers, and other industrial products.
That was not a small fight.
He was pushing against powerful industrial interests. Caltech notes that Patterson’s work put him at odds with major industry lobbies and that he paid a professional price for it.
That matters.
Because Patterson is a reminder that systems can be wrong for a long time.
They can protect harmful practices.
They can dismiss inconvenient evidence.
They can make life difficult for the people pointing out the problem.
But occasionally, someone keeps pushing anyway.
Major General Sir Robert Risson did that for Melbourne’s trams.
Clair Patterson did that for environmental lead.
Different countries. Different issues.
Same pattern.
Society benefits when individuals are willing to resist powerful interests, even when it costs them personally.
So what does this have to do with magnets?
This is where my recent trip to the United States ties back to Q Magnets.
At Maryville University, I spoke with Professor Dr Pradip Ghosh and final-year physiotherapy students who had completed a small knee osteoarthritis study using quadrapolar Q Magnets.
Another group was preparing to begin a lower back pain study.
We had a very useful discussions about research design, patient compliance, placement, dosage, outcomes, placebo effects, and what can realistically be measured.
And that is exactly where this subject belongs.
Not in hype.
Not in miracle claims.
But in careful observation.
The knee pain study
The first group looked at knee osteoarthritis.
They used an A–B–A design:
• baseline testing
• three weeks using the magnets
• three weeks without the magnets
• then three weeks using them again
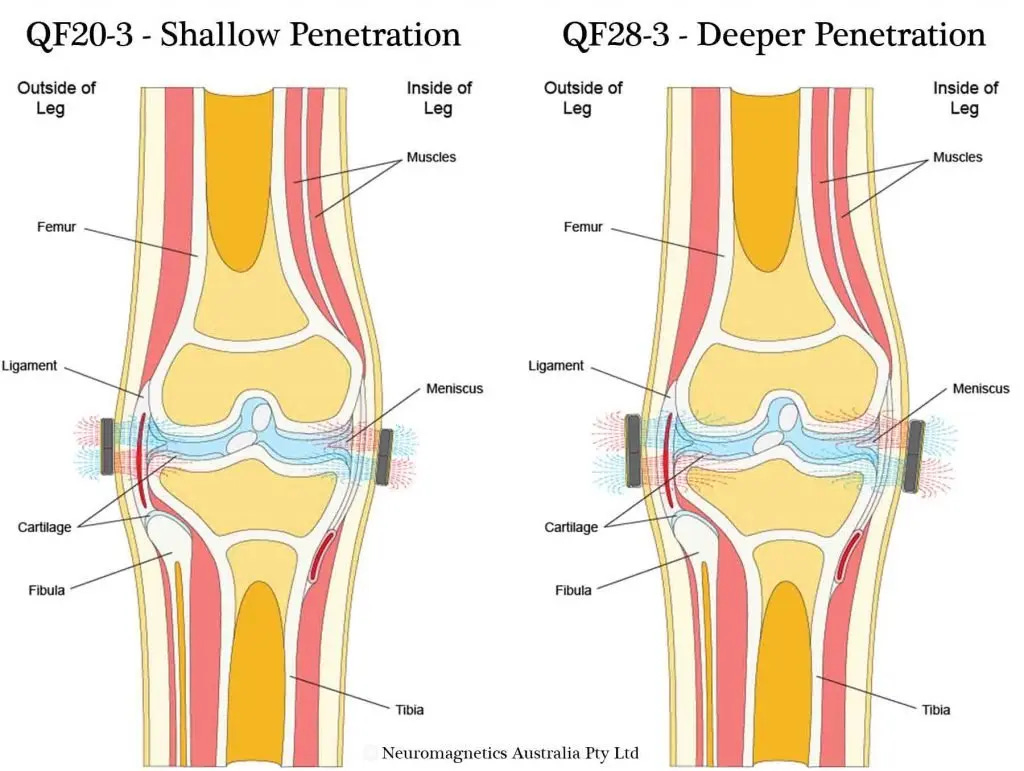
Participants wore the magnets for two hours a day, five days a week. They were placed on the medial and lateral sides of the tibiofemoral joint line. Following the Q Magnets protocol for knee pain.
The students measured outcomes using gait data, the visual analogue scale for pain, and the KOOS knee osteoarthritis outcome score.
The most interesting finding was not simply “pain went down.”
Pain scores were mixed.
But function changed.
Step length improved during the magnet phases, and in several participants it declined when the magnets were removed. Gait velocity and KOOS scores also improved when compared with baseline.
One of the students made a point that I think is worth remembering:
“We didn’t have a single patient who said this was not beneficial for me… the subjective reports of improvement were there across the board.”
That is not definitive proof.
But it is a signal.
And in healthcare, signals are often where better questions begin.
The lower back pain study
The second group was preparing a study on chronic lower back pain.
This discussion was especially useful because it showed how difficult good research can be.
Where should the magnets be placed?
Should placement be standardised across every participant?
Or should it be based on the individual’s symptoms, anatomy, and pain presentation?
If someone’s issue is at L5–S1 but the study protocol places the magnet at L4–5, then you may have the right field and the right duration, but the wrong placement.
That matters.
Because with Q Magnets, the question is rarely as simple as:
“Do magnets work?”
A better question is:
“Under what conditions do they influence biology?”
That means considering:
• Field — strength, gradient, and configuration
• Dose — duration and consistency
• Placement — anatomical relevance
• Context — condition, timing, and tissue state
This framework sits at the heart of MagnaBlog’s approach: avoid binary thinking and focus instead on when, where, and why static magnetic fields may influence outcomes.
Why many therapies are misunderstood
This is where the system problem returns.
Modern healthcare often favours interventions that are easy to standardise, patent, fund, and scale.
That does not automatically make those interventions bad.
But it does mean other approaches may struggle to gain attention, especially if they require careful application, clinician judgement, or individualised placement.
Q Magnets are not a drug.
They are not a procedure.
They are not a one-size-fits-all intervention.
They depend on use.
They depend on placement.
They depend on the right magnetic field for the right tissue and condition.
That makes them harder to study, but not less worthy of study.
In fact, it makes the research more important.
The wrong conclusion is the easiest one
When people hear “magnets,” many already have an opinion.
Some think of fridge magnets.
Some think of weak flexible magnetic products that were poorly designed.
Some think of pseudoscience.
That history has muddied the water.
But poor products and poor explanations do not mean the entire field should be dismissed.
A badly designed tram system does not prove public transport is useless.
A weak magnetic product used in the wrong place does not prove static magnetic fields have no biological relevance.
The design matters.
The placement matters.
The dose matters.
The context matters.
What I took from the United States
My recent trip reminded me of two things at once.
First, large systems often protect what already has influence.
That is true in politics.
It is true in transport.
And it is true in healthcare.
Second, progress often starts with individuals who are willing to ask better questions before the system is ready to accept them.
Researchers.
Practitioners.
Students.
Patients.
People who notice something, test it, refine it, and keep going.
That is how many useful ideas begin.
Not as accepted wisdom.
But as careful observation.
The practical takeaway
When looking at any intervention, including Q Magnets, the better question is not:
The better questions are:
• What type of field is being used?
• Where is it placed?
• How long is it worn?
• Is it being used consistently?
• What condition is being treated?
• What outcome is being measured?
That is where useful understanding begins.
Final thought
History shows that society does not always adopt the best ideas first.
Sometimes it adopts what is profitable.
Sometimes it adopts what is politically convenient.
Sometimes it adopts what powerful interests are willing to support.
But not always.
Sometimes, courageous people resist.
Clair Patterson pushed back against the lead industry.
Major General Sir Robert Risson helped preserve Melbourne’s trams.
And today, in a much smaller but still meaningful way, practitioners and researchers are asking better questions about Q Magnets.
That is how progress often begins.
Not with hype.
Not with certainty.
But with careful observation, practical testing, and the willingness to keep asking:
Under what conditions does this help?
Until next time, stay curious and stay well,
James Hermans
and the Q Magnets Team
The Weekly Reframe
A short thought to carry into the week.
“You don’t stop exercising because you get old; you get old because you stop exercising.” — Dr Ross Walker, Cardiologist
Featured Article
How Rockefeller’s Flexner Report Suppressed Electric & Magnetic therapy

The irrational and remarkable bias against the therapeutic use of static magnets
Field. Dose. Placement. The science behind effective magnetic field therapy.

Chlorine dioxide. Have you heard of it?
It may be one of the many suppressed, yet highly effective therapies.
See discussion by Dr Pierre Kory here on x.com...
https://x.com/dawnsmission/status/2052728713842717112?s=58&t=iI-31sZiFdz7_fpIExq1VA